Marshall syndrome
| Marshall syndrome | |
|---|---|
| Other names: Deafness, myopia, cataract, saddle nose-Marshall type [1] | |
 | |
| Marshall syndrome and Stickler syndrome is inherited in an autosomal dominant pattern. | |
Marshall syndrome is a genetic disorder of the connective tissue[2] which can cause hearing loss. The most common areas to be affected are the eyes which are uncommonly large, joints and the mouth and facial structures[3][4].
Marshall syndrome and Stickler syndrome closely resemble each other; in fact they are so similar, one may be a subset of the other[5]
Signs and symptoms

- Eyes-Myopia is a common eye problem in Marshall syndrome; cataracts also occur more frequently and detached retina less frequently. Myopia also is also a common problem with the eyes in Stickler syndrome; in the latter syndrome, extreme myopia may lead to severe eye problems such as detached retina.[6][7][8]
- Joints-The joint changes include hyperextensibility (double-jointedness) and arthritis. Babies and young children with Stickler syndrome usually have very hyperextensible joints, as an affected child gets older, they may experience pain and stiffness from overuse of a joint. Osteoarthritis of the large joints often develops during the third or fourth decade. The joint changes in Marshall syndrome are of the same type but to a lesser degree, there also may be changes in the bones that show up on X-ray but generally are not a problem.[6][1][9][8]

- Orofacial Structure-The most severe problem associated with Stickler syndrome is Pierre Robin syndrome. This refers to a cleft palate resulting from a very small lower jaw. During early fetal life, the roof of the mouth is normally open and the sides of the palate have to come together to close. If the jaw is too small, there is not enough room for the tongue which is then pushed up and gets in the way of the closing palate; sometimes the chin is so small the baby has problems with eating and breathing if the tongue blocks the back of the throat.The facial features of Marshall Syndrome include a flat midface, the appearance of large eyes, short upturned nose, and a round face.[3][7][8][10][6]
- Hearing loss-Sensorineural hearing loss has been reported as severe and as low as mild in affected individuals. A conductive loss due to otitis can magnify an existing sensorineural loss and is a frequent problem for children with Stickler or Marshall Syndrome.[1][7][6]
Genetics

One finds that this condition is due to mutations in collagen XI, alpha-1 polypeptide COL11A1 gene, which is located on chromosome 1p21.1.[6][11]Stickler syndrome and Marshall syndrome both have an autosomal dominant pattern of inheritance, however, there is alot of variation within and among families with regard to gene expression.[6]
Some may be more severely affected and others may be very mildly affected, often these syndromes are not recognized in a family until a baby is born with Pierre Robin syndrome or some members have detached retinas or cataracts at a young age.[6][7][5]
COL11A1
COL11A1 gene provides information to create a part of pro-alpha1(XI) chain. Type XI collagen is found in cartilage in the human body.In Marshall syndrome a segment of DNA of the COL11A1 gene is skipped hence an abnormally short pro-alpha1(XI) chain. [12]
Diagnosis
Diagnosis is made based on features as well as by the very early onset of serious eye and ear disease. Because Marshall syndrome is an autosomal dominant hereditary disease, physicians can also note the characteristic appearance of the biological parent of the child. There are no tests for Stickler syndrome or Marshall syndrome. It is an area of active research, also the genetic testing being expensive supports that the diagnosis is made depending on the features.[7][1][6]
Differential diagnosis
The DDx for this condition, Marshall syndrome is based on the following:[6]
- Stickler syndrome type 2
- Wagner syndrome
- Congenital syphilis
- Congenital spondyloepiphyseal dysplasia
Treatment

There is no medical treatment for either syndrome but there are some recommendations that can help with prevention or early identification of some of the problems. Children with either syndrome should have their hearing tested, and adults should be aware that the hearing loss may not develop until the adult years. Yearly visits to an ophthalmologist or other eye care professional who has been informed of the diagnosis of Stickler or Marshall syndrome is important for the affected individual. Children should have the opportunity to have myopia corrected as early as possible, and treatment for cataracts or detached retinas may be more effective with early identification. [9][6]
Prognosis
In terms of the prognosis for Marshall syndrome has medical literature indicating individuals who are in their 30s and 40s, and may have a normal life expectancy. However the severity of symptoms may affect different individuals differently.[1]
Epidemiology
Marshall syndrome affects both men and women equally[6]
Research
Research is needed in terms of IOL implantation in the lens capsule for the affected lens in children with congenital cataract[6]
Additional images
-
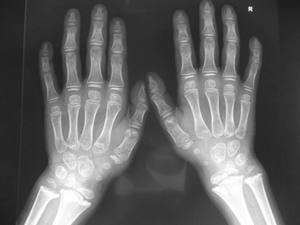
( Marshall-Stickler overlap) Anteroposterior hand radiograph showed, short-stubby hand with large carpal bones associated with pseudoepiphyses of a joint.
-
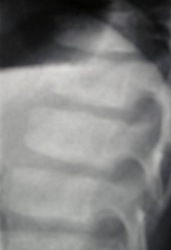
Lateral spine radiograph showed platyspondyly associated with anterior clefting of the vertebrae.
-

( Marshall-Stickler overlap) Anteroposterior pelvis radiograph showed, coxa valga, a hypoplastic ileae, acetabulo-femoral and metaphyseal dysplasia




References
- ↑ 1.0 1.1 1.2 1.3 1.4 "Marshall syndrome | Genetic and Rare Diseases Information Center (GARD) – an NCATS Program". rarediseases.info.nih.gov. Archived from the original on 20 June 2019. Retrieved 20 June 2019.
- ↑ James, William; Berger, Timothy; Elston, Dirk (2005). Andrews' Diseases of the Skin: Clinical Dermatology (10th ed.). Saunders. pp. 146–7. ISBN 0-7216-2921-0.
- ↑ 3.0 3.1 "Marshall syndrome - Conditions - GTR - NCBI". www.ncbi.nlm.nih.gov. Archived from the original on 30 July 2017. Retrieved 23 September 2021.
- ↑ RESERVED, INSERM US14-- ALL RIGHTS. "Orphanet: Marshall syndrome". www.orpha.net. Archived from the original on 18 September 2020. Retrieved 21 September 2021.
- ↑ 5.0 5.1 Valdes, Ana M. (1 January 2018). "Chapter 24". Genetics of Bone Biology and Skeletal Disease (Second Edition). Academic Press. pp. 421–438. ISBN 978-0-12-804182-6. Archived from the original on 26 September 2021. Retrieved 29 September 2021.
- ↑ 6.00 6.01 6.02 6.03 6.04 6.05 6.06 6.07 6.08 6.09 6.10 6.11 "Marshall Syndrome". NORD (National Organization for Rare Disorders). Archived from the original on 25 February 2021. Retrieved 21 September 2021.
- ↑ 7.0 7.1 7.2 7.3 7.4 "OMIM Entry - # 154780 - MARSHALL SYNDROME; MRSHS". omim.org. Archived from the original on 1 April 2021. Retrieved 24 September 2021.
- ↑ 8.0 8.1 8.2 "Stickler Syndrome". NORD (National Organization for Rare Disorders). Archived from the original on 1 April 2021. Retrieved 17 October 2021.
- ↑ 9.0 9.1 "Stickler syndrome | Genetic and Rare Diseases Information Center (GARD) – an NCATS Program". rarediseases.info.nih.gov. Archived from the original on 19 August 2021. Retrieved 5 October 2021.
- ↑ "Facts about Cleft Lip and Cleft Palate | CDC". Centers for Disease Control and Prevention. 28 December 2020. Archived from the original on 8 May 2015. Retrieved 20 October 2021.
- ↑ "Marshall syndrome (Concept Id: C0265235) - MedGen - NCBI". www.ncbi.nlm.nih.gov. Archived from the original on 17 October 2021. Retrieved 16 October 2021.
- ↑ "COL11A1 gene: MedlinePlus Genetics". medlineplus.gov. Archived from the original on 24 March 2021. Retrieved 10 October 2021.
External links
| Classification | |
|---|---|
| External resources |