License
Attribution 4.0 International (CC BY 4.0)
Summary
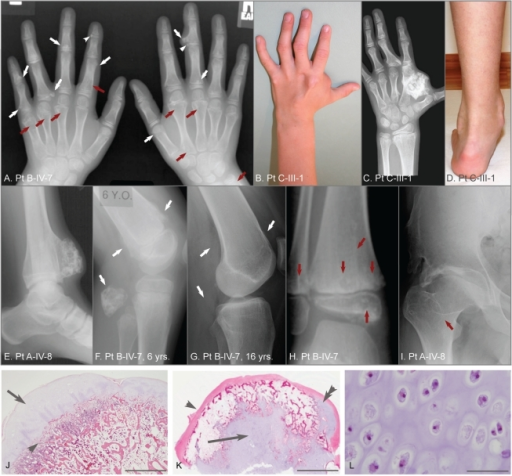
Author:Bowen ME, Boyden ED, Holm IA, Campos-Xavier B, Bonafé L, Superti-Furga A, Ikegawa S, Cormier-Daire V, Bovée JV, Pansuriya TC, de Sousa SB, Savarirayan R, Andreucci E, Vikkula M, Garavelli L, Pottinger C, Ogino T, Sakai A, Regazzoni BM, Wuyts W, Sangiorgi L, Pedrini E, Zhu M, Kozakewich HP, Kasser JR, Seidman JG, Kurek KC, Warman ML,Department of Orthopaedic Surgery, Children's Hospital Boston and Harvard Medical School(Openi/National Library of Medicine) Source:https://openi.nlm.nih.gov/detailedresult?img=PMC3077396_pgen.1002050.g001&query=Metachondromatosis&it=xg&req=4&npos=3 Description:pgen-1002050-g001: Clinical, radiographic, and histologic features of metachondromatosis.(A) Hand radiographs of participant B-IV-7, taken when 8-years-old. Exostotic lesions (white arrows) are present in the phalanges and metacarpals, and arise from the metaphysis (arrows) or epiphysis (arrowheads). Exostoses tend to point toward the adjacent joint. Endosteal lesions (red arrows) cause metaphyseal expansion. (B, C, D) Hand photograph and radiograph, and foot photograph of participant C-III-1 taken when 9-years-old, depicting mild shortening and deformity of the digits, a large exostotic lesion arising from the second metacarpal bone in the hand, and ankle enlargement superior to the malleoli due to exostoses of the tibia and fibula. (E) Ankle radiograph of participant A-IV-8 taken when 19-years-old depicting a recurrence of a previously excised exostotic lesion of the distal tibia that spans the physis. (F, G) Lateral knee radiographs of participant B-IV-7, taken at 6 years and 16 years, respectively. Note that multiple exostotic lesions of the distal femur and proximal fibula (white arrows) seen when 6-years-old (F) have regressed in the absence of surgical intervention by 16-years of age (G). (H) Ankle radiograph of participant B-IV-7, taken when 5-years-old, demonstrating radiolucency associated with endosteal lesions (red arrows) in the tibia and fibula, and mild metaphyseal flaring. Despite combined metaphyseal and epiphyseal involvement, this individual's linear growth was not affected. (I) Hip radiograph of participant A-IV-8 taken when 22-years-old depicting an endosteal lesion of the femoral neck (arrow) that has caused degeneration of the femoral head and spurring of the acetabulum. (J) Low power photomicrograph of an hematoxylin and eosin (H&E) stained section through an exostosis that had been excised from a patient with hereditary multiple exostoses. Note this exostosis is a typical osteochondroma, having a well-developed surface cartilaginous cap (arrow) and endochondral bone immediately below (arrowhead). The scale bar represents 0.15 cm (K) Photomicrograph of an H&E stained exostotic lesion excised from participant A-IV-5 when 5-years-old. This lesion is predominantly covered by a fibrous cap (arrow) and has only a small, eccentric cartilaginous cap (double arrowhead). The majority of cartilage in this, and in 14 other exostoses from patients with MC that have been analyzed, is found within a central core (arrow) and has bone formation occurring at the periphery of this cartilage core. The scale bar represents 0.5 cm. (L) High-power image of the central cartilage core shows chondrocytes with prominent cytoplasm no organization typical of a growth plate. The scale bar represents 100 µm.
{kind=link}
{kind=link}