Bowel-associated dermatosis–arthritis syndrome
| Bowel-associated dermatosis–arthritis syndrome | |
|---|---|
| Other names: Bowel bypass syndrome and Intestinal bypass arthritis–dermatitis syndrome | |
 | |
| Pustules and crusts around the elbows in a patient with Crohn's disease and bowel-associated dermatosis-arthritis syndrome (BADAS) | |
| Specialty | Dermatology |
Bowel-associated dermatosis–arthritis syndrome (BADAS), is a complication of jejunoileal bypass surgery consisting of flu-like symptoms (fever, malaise), multiple painful joints (polyarthralgia), muscle aches (myalgia) and skin changes. It has been reported to occur in up to 20% of patients who had jejunoileal bypass surgery, a form of obesity surgery that is rarely performed today.[1]
An excessive immune response to gut bacteria is thought to cause BADAS. Antibiotics have been used successfully to treat the condition (including tetracyclines, macrolides, metronidazole and fluoroquinolones). Corticosteroids are an alternative. Surgical repair of the normal bowel transit, where possible, can be effective.
BADAS has later been reported in patients with inflammatory bowel disease,[1] diverticulitis[2] and following resection of the stomach (gastrectomy). BADAS has also been reported following biliopancreatic diversion (a form of bariatric surgery, also known as Scopinaro procedure),[3] and in one case, BADAS occurred in a patient with acute appendicitis.[4] Since "bowel bypass syndrome" is not applicable to these cases, the term BADAS was coined by Jorizzo and co-authors in 1984.[1]
Symptoms and signs
The most typical skin changes are a red patch (erythematous macula) with a central vesicle or pustule that heals without scarring. This maculopapular rash can recur every 4–6 weeks and predominantly affect the upper chest and arms. Erythema nodosum-like skin lesions can affect the legs. When a skin biopsy is examined under the microscope, there can be signs of a neutrophilic dermatosis. The joint pains in BADAS are typically episodic, migratory and affecting multiple joints. They can affect the small joints (e.g. interphalangeal joints of the fingers) and there can be associated tenosynovitis, but there is no erosion or deformation in the long term.
-

Scattered hemorrhagic vesicles
-
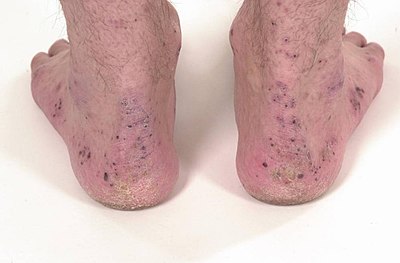
Crusts around the ankles and feet in the same patient as above
.png)

Mechanism
Immune complexes are thought to cause blood vessel damage, attracting neutrophils into the skin and synovium in BADAS.[6] These antigen-antibody complexes are thought to be caused by excessive exposure to bacterial antigens (especially peptidoglycans).[7] Bacterial overgrowth appears to be a frequent underlying condition. These antibodies possibly stimulate migration of neutrophils into the affected joints and skin. The effect of antibacterial therapy supports a role for bacteria in the disease mechanism (pathogenesis).
Diagnosis
Differential diagnosis
The DDX for this condition is as follows:[8]
- Subacute bacterial endocarditis
- Systemic candidiasis
- Behcet's disease
Treatment
The management of this condition, Bowel-associated dermatosis–arthritis syndrome, can be done via antibiotics and dapsone[9]
See also
References
- ↑ 1.0 1.1 1.2 Jorizzo JL, Apisarnthanarax P, Subrt P, et al. (March 1983). "Bowel-bypass syndrome without bowel bypass. Bowel-associated dermatosis-arthritis syndrome". Arch. Intern. Med. 143 (3): 457–61. doi:10.1001/archinte.143.3.457. PMID 6830382.
- ↑ Brouard MC, Chavaz P, Borradori L (January 2004). "Acute pustulosis of the legs in diverticulitis with sigmoid stenosis: an overlap between bowel-associated dermatosis-arthritis syndrome and pustular pyoderma gangrenosum". J Eur Acad Dermatol Venereol. 18 (1): 89–92. doi:10.1111/j.1468-3083.2004.00712.x. PMID 14678541.
- ↑ Slater GH, Kerlin P, Georghiou PR, Fielding GA (January 2004). "Bowel-associated dermatosis-arthritis syndrome after biliopancreatic diversion". Obes Surg. 14 (1): 133–5. doi:10.1381/096089204772787446. PMID 14980049.
- ↑ Prpić-Massari L, Kastelan M, Brajac I, Cabrijan L, Zamolo G, Massari D (August 2007). "Bowel-associated dermatosis-arthritis syndrome in a patient with appendicitis". Med. Sci. Monit. 13 (8): CS97–100. PMID 17660731.
- ↑ Rapini, Ronald P.; Bolognia, Jean L.; Jorizzo, Joseph L. (2007). Dermatology: 2-Volume Set. St. Louis: Mosby. ISBN 978-1-4160-2999-1.
- ↑ Jorizzo JL, Schmalstieg FC, Dinehart SM, et al. (April 1984). "Bowel-associated dermatosis-arthritis syndrome. Immune complex-mediated vessel damage and increased neutrophil migration". Arch. Intern. Med. 144 (4): 738–40. doi:10.1001/archinte.144.4.738. PMID 6712372.
- ↑ Ely PH (June 1980). "The bowel bypass syndrome: a response to bacterial peptidoglycans". J. Am. Acad. Dermatol. 2 (6): 473–87. doi:10.1016/S0190-9622(80)80148-4. PMID 7400404.
- ↑ Bolognia, Jean L.; Jorizzo, Joseph L.; Rapini, Ronald P. Dermatology. Gulf Professional Publishing. p. Google books does not offer page. ISBN 978-99976-38-99-1. Archived from the original on 2 November 2021. Retrieved 2 November 2021.
- ↑ Bayless, Theodore M.; Hanauer, Stephen B. (2001). Advanced Therapy of Inflammatory Bowel Disease. PMPH-USA. p. 273. ISBN 978-1-55009-122-9. Archived from the original on 2 November 2021. Retrieved 2 November 2021.